Search Here
Every 13 minutes, a woman dies from breast cancer. Unfortunately, many women with the disease do not show symptoms. So, regular screening for breast cancer is critical for early detection and diagnosis.
Breast Cancer screening typically occurs as a part of routine preventative care. Individuals do not have to have any signs or symptoms to have a screening performed by their doctor. Manual exams, ultrasound, thermography, and mammography are a few ways patients are screened for abnormalities. A doctor can explain screening options and when it is time to consider certain tests.
To find out how breast cancer screening aids in the diagnosis of the disease, read on.

Breast cancer can be asymptomatic. In other words, it may have no symptoms. In fact, cases may show different symptoms and examination findings. That is why screening should be individualized for each patient.
Screening means looking for or testing for something when there are no signs.
Many people think that only someone with a family history should worry. Yet, about 85% of breast cancers occur in women who do not have any family history of breast cancer. Rather, genetic mutations that occur as women age increase their risk. The most significant risk factors for breast cancer are being a woman and growing older.
Doctors are trained in the latest research and guidelines. They can tell their patients about the options. And doctors help women decide when it is a good idea to be tested.
Breast cancer is typically diagnosed in one of the following ways:
Mammography is the most common screening method used today. Other testing methods include Digital Breast Tomosynthesis (DBI) and thermography, although these are not widely used.
According to a recent article, doctors are seeing later-stage cancer cases in younger women. This is worrisome because cancers detected in younger women in their 20s and 30s are more aggressive. And they may lead to poorer outcomes.
Doctors are seeing later-stage cancer cases in younger women. This is worrisome.
Early detection is key in cancer treatment. The cost of treatment, risks of complications including death, and length of treatment go down with earlier detection.
If not caught early, cancers can grow and spread. When cancer cells move to other organs, this is called metastasis. Thus, cancer is harder to treat.
The best way to catch cancerous changes early is through regular check-ups with a doctor and routine screening tests to help detect changes early. Online doctors or virtual gynecologists can order mammograms or other imaging tests, and tailor screening plans for women who do not usually see a primary care physician.
Medical researchers continue to look for ways to help doctors with better and more accurate tests.
In 2019, the National Cancer Institute presented a new study that showed Doctors could detect breast cancer up to five years before any clinical signs appear, using a blood test for tumor-associated antigens (TAAs).
Newer research from Johns Hopkins University School of Medicine paired blood tests with other screening tests to determine whether finding and treating cancers identified by blood tests reduced mortality rates. Researchers said that “some screening may actually cause more harm than good.” And so, they used bloodwork with standard imaging procedures.
Results were promising. Researchers concluded that there is hope for a blood test that could eventually reduce deaths from cancers that typically go undetected until late stages. But “any blood test needs to complement and add to standard-of-care screening because standard-of-care screening works.”
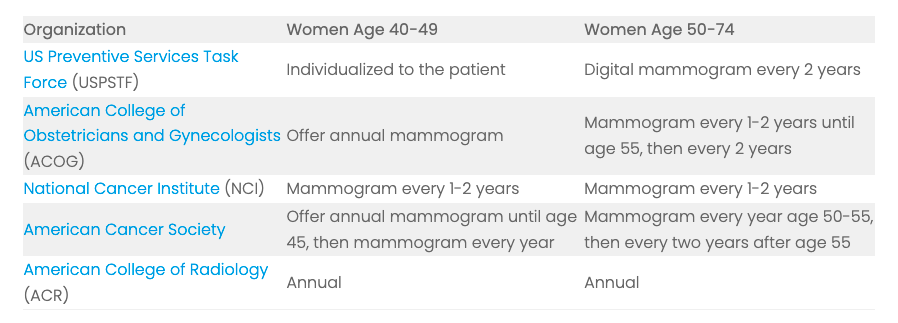
Current recommendations encourage most women to have a mammogram beginning at age 40. Here are the most recent guidelines on screening.
My Virtual Physician can offers virtual gynecology services in many states. Women can talk with experts about individualized screening plans. Don’t worry about your risk. Talk to the doctor now.
My Virtual Physician is now accepting new patients.
Stefanie (00:00):
The information presented in this podcast is offered for educational purposes, only presenting it is not intended to and does not create a provider-patient relationship between any presenter and anyone else about the medical topics addressed presenters provide general information only not diagnosis or recommended treatments or any other information specific to any individual listeners are encouraged to see their own healthcare professional about all topics address on talk Tuesdays or for any other medical problem. [inaudible] welcome everyone. Thank you for joining us today. My name is Stefanie and I'm part of the team here at My Virtual Physician. We are a direct to consumer multi-specialty telemedicine provider operating in multiple States. It is Talk Tuesday and we are continuing our weekly educational series to talk with our experts, explore some common healthcare concerns that we see and hopefully answer some questions you may have today. Our physician expert is Dr. Coleman. She is a general surgeon, and today we are going to talk about breast cancer surgery. So thank you
Dr. Ginger Coleman (01:14):
Joining us today. Thanks for having me. Yeah. And welcome back. Okay. So after the biopsy, they told me that I have cancer. So now what, so there's a bunch of different types of cancer. So the first thing will depend on what kind of cancer you have and how big it is, and if lymph nodes are involved. So, so don't panic, there's, there's a lot of options for surgery and every option would be something that you would need to discuss with your personal physician and determine what the best course of action is for you and your particular type of cancer. But, but we'll discuss a couple common options. Um, there's something called breast conservation surgery also known as a lumpectomy or a partial mastectomy. So this is where a small ish incision is made. It's not necessarily right over where the area of cancer is. We try and hide the incisions.
Dr. Ginger Coleman (02:22):
So sometimes we may put it around the nipple. Sometimes we may put it and underneath the breast, sort of in the, in the fold, sometimes we gotta just make an incision across your skin and we try and hide it as best as we can, but it doesn't happen all the time. Essentially, once we make that incision, we remove a small portion of breast where the cancer is as well as some normal breast tissue surrounding it. And in order to do that, because if you had a lesion that wasn't palpable, it was just something abnormal seen on your mammogram. Obviously, we can't it in the, or so we have to have our radiologists localize it for us, what used to be done. And it's still done in a lot of places, but we're moving away from it is what's called a wire localization and you would go to mammography before surgery.
Dr. Ginger Coleman (03:20):
The radiologists would do another mammogram and they would find that area of concern. And then they stick a little wire into the lesion. So we're trying to get away from it because it's not real fun to be wheeled around the hospital with a wire sticking out of your breast, waiting to go to surgery. But that wire is directed to that area where you have cancer or the area of concern that needs to be removed. And they give us mammogram images to use in the operating room to make sure that we know where that is. So, so we'll excise that area more recently, they've moved to using things like radioactive seeds that can be placed by the radiologist and they can, they can be done a couple of days before surgery, some even up to a couple of weeks before surgery. So it's not something you have to come in that day and get done.
Dr. Ginger Coleman (04:10):
You can get it done kind of on your own time, leading up to surgery. And then in the operating room, we use a little, I call it the Geiger counter, but it's a little probe that beeps when you get close to the, the seed or, or whatever it is that they used, there's a whole bunch of different kinds. And, and so that helps locate the area of cancer. And then that gives us an idea and we remove that portion of tissue. And then, like I said, some normal breast tissue around it. And depending on the type of cancer you have will determine how much breast tissue we need to take. And depending on, you know, if you have DCIS or you have invasive cancer, that will also determine if we need to take any lymph nodes from your XLO also known as your armpit. Okay.
Dr. Ginger Coleman (04:59):
So then you said there were more than one type. So what's the other. Yes. And the other type is a mastectomy and that's where your whole breast is removed. There are different types of mastectomies. A simple mastectomy is probably what most people are familiar with. And that would be where all of your breast tissue and your nipple and areola are removed. And you have just a flat chest after that, on that side, there's something called a modified radical mastectomy. And that's a simple mastectomy, except during this operation, all of the lymph nodes in your Exela are removed that's surgery. There's some other mastectomies, a nipple-sparing mastectomy, and skin-sparing mastectomies that are also options. I won't really go into those, but, but really any mastectomy that's done can be followed with breastfeeding plastic surgeon, either during the same operation or at a later date. It all depends on the type of cancer you have and what other treatments that you need after surgery and understanding that there are risks and benefits of each type of surgery and what may be best for you may not be, you know, what you really desired to have done. There's if you need radiation after having a mastectomy, you don't really want to have reconstruction because you're not going to heal and you're going to have more problems and need more surgery. You may not have any complications, but do you want to risk it? So even after a mastectomy, you can get reconstruction, you can get it done that day, and we do that pretty frequently, but it all depends on you in particular, what's going on with you and what treatments that you need.
Stefanie (06:59):
Yeah. Um, so then you S you said lymph nodes. And can you talk to us a little bit about that or why they're removed?
Dr. Ginger Coleman (07:08):
Yeah. So your lymph nodes often are, are said to quote unquote, filter your blood. And so if you have breast cancer that is going to drain into your lymphatic system, and we'll go through those lymph nodes. And usually if you have breast cancer on the right side, you look in the right armpit for the lymph nodes and see if you can feel any that are, you know, big or thick and kind of mad at or anything. And even if they feel normal, it doesn't mean that there's not tumor in them. So if you find tumor in those lymph nodes, it's a sign of metastatic disease and it's more affiliated with invasive cancer. And so that's why it's important for us to evaluate the women, especially in invasive cancer. And you can do it in two ways. Again, there's two ways, there's something called a Sentinel lymph node biopsy, or you can have an auxiliary dissection.
Dr. Ginger Coleman (08:07):
So with a Sentinel lymph node biopsy, you can do this with either breast conservation or a mastectomy. If you do it with breast conservation, it's a separate incision, and it's not real big. We try and hide it in the, you know, one of the creases in your armpit or at the hairline, just to kind of hide the scar, but it is a separate incision. And we go through there to find the lymph nodes. If you do the lymph node biopsy with a mastectomy, it's all through the same incision. So you don't have two separate incisions prior to surgery. You usually go to a nuclear medicine department and get this radioactive tracer injected. And then in the operating room, we use a blue dye, methylene blue. I just often blue something and we inject and everyone does it a little bit different, but we always injected it underneath the nipple, or I'm sorry, underneath Ariel.
Dr. Ginger Coleman (09:03):
And then you do your surgery and, and the axilla is the last thing that you do. So by the time you get there, hopefully all that blue dye has made it swaying to your lymph nodes. And so we use that little Geiger counter thing again, and it helps you find that radioactive tracer, but then we're also looking for blue. So what we want to do is find the blue and radioactive lymph nodes and remove those. And the machine will give you a number and you want to take the highest number because that's theoretically the lymph node that drained first or the Sentinel node. And we usually take about three more or less. It kind of depends on what we see in there. If it's very obvious that all of your lymph nodes are involved, you may then end up with an axillary dissection and not just the Sentinel lymph node biopsy.
Dr. Ginger Coleman (09:57):
So an axillary dissection is actually where all of the lymph nodes are removed. Usually we do this with a mastectomy, so like the modified radical mastectomy, and it's all through the same incision. Sometimes you can do it after a lumpectomy or any other surgery that you've had, or Sentinel lymph node biopsy. If that biopsy came back with signs of invasive cancer that eat, that indicated you you'd need all of the lymph nodes removed. So then we would have to go back and do another operation, but usually we do it with a mastectomy. So it's all one surgery. And we just take out all of those lymph nodes. There are some nerves and blood vessels in the area that are important that we don't disrupt. They can cause some, you know, numbness or tingling of your arm or difficulty moving your shoulder, or even make your shoulder blades stick out.
Dr. Ginger Coleman (10:56):
But injuries to those nerves are not really common. Okay. So then you did your mastectomy or lumpectomy. So what happens after surgery? So depending on the type of surgery you had, you'll either go home that day or you'll stay overnight in the hospital. And usually nobody has to stay more than 23 hours or no more than a day. If you, if you had a lumpectomy and you don't have any serious medical conditions or anything that would be of concern, usually you just go home. So someone will, someone will need to drive you home. And we'll see you in clinic in a couple of weeks and let you know the pathology. If you had a mastectomy, you usually stay in the hospital, at least overnight, uh, you will have a drain or two, depending on if you had to have an axillary dissection or not. Um, and, and every surgeon is different with how they do it, but, but usually you will have at least wondering.
Dr. Ginger Coleman (11:58):
So we'll teach you how to take care of that. We keep you overnight to make sure that there's not a lot of bleeding out of the drain or anything that would be concerning to need to take you back surgery. Uh, if you do, okay, you go back home and then you see us in clinic and we'll take the drains out in clinic and talk about pathology. Uh, and, and if you haven't seen an oncologist already, we'll send you to one. Um, usually they're the ones that send you to us. So that's, that's usually pretty well organized, but that's when you would talk with them about the need for chemo or radiation. And sometimes if, you know, we do breast conservation surgery and maybe we didn't get all of the cancer, it'll be called, you know, you have positive margins. And so at that time, we would have to talk about going back for either re-excision of those areas that were positive and depending on your breast size and the type of cancer you have and all of that, it, it may end up being okay, well, now we need to talk about actually doing mastectomy because the pathology showed whatever it showed, but there is a possibility that you, that you would have to go back to surgery if you do breast conservation.
Dr. Ginger Coleman (13:15):
And it doesn't happen all the time, but it is, you know, one of the risks of trying to preserve the breast tissue.
Stefanie (13:23):
Um, thank you so much, dr. Coleman. I know it's a really hard topic to talk about. Cancer is always something that's pretty scary word. I appreciate you joining us for Talk Tuesday and telling us what we need to know about breast cancer screening and breast cancer surgery for everyone else. Joining us as well. This has been Talk Tuesdays with my virtual physician. You can schedule a consultation with one of our doctors by visiting our website at www.myvirtualphysician.com. We look forward to seeing you again, and we hope you have a great week Nation presented in this podcast is offered for educational purposes, only presenting it is not intended to and does not create a provider-patient relationship between any presenter and anyone else about the medical topics addressed presenters provide general information only not diagnosis or recommended treatments or any other information specific to any individual listeners are encouraged to see their own healthcare professional about all topics address in Talk Tuesdays or for any other medical problems.
Speaker 1:
The information presented in this podcast is offered for educational purposes, only presenting it is not intended to and does not create a provider-patient relationship between any presenter and anyone else about the medical topics addressed presenters provide general information only not a diagnosis or recommended treatments or any other information specific to any individual listeners are encouraged to see their own health care professional about all topics address on Talk Tuesdays or for any other medical problem.
Speaker 1:
Welcome, everyone. Thank you for joining us today. My name is Stephanie and I'm part of the team here at My Virtual Physician. We are a direct to consumer multi-specialty telemedicine provider operating in multiple States. It is Talk Tuesday and we are continuing our weekly educational series to talk with our experts, explore some common healthcare concerns that we see and hopefully answer some questions you may have today. Our physician expert is dr. Coleman. She is a general surgeon, and today we are going to talk about breast cancer screening and breast cancer surgery. So thank you for joining us today. Thanks for having me. Yeah. And welcome
Speaker 2:
Back October was breast cancer awareness month. So we're going to be doing
Speaker 1:
Again a blog and an episode or two of Talk Tuesday on breast cancer screening. When would someone go in to get a mammogram or if they feel something or they have any history of breast cancer in their family, what's kind of the age range,
Speaker 2:
What to look for. Okay. So there's actually three organizations, probably more, but there's at least three organizations that have opinions on breast cancer screening, depending on which organization you listen to, it could be 40 years old, 45 years old or 50 years old, either way. Everyone agrees that by the age of 50, you should be getting a screening mammogram, most people, uh, and I believe most insurance companies go with the age of 40 breast cancer. Under the age of 40 is pretty rare. If, if you have
Speaker 1:
Breast cancer under the age of 40, usually it's associated
Speaker 2:
With some sort of genetic predisposition. There's the BRC mutation that predispose people to, to breast cancer at a younger age. But there's some other things that can, can run in families. Some other genetic diseases that predispose you at a younger age and typically cancer at a younger age is more aggressive and more advanced when it's found, because who in their thirties thinks that they're going to have breast cancer. So what we learned in residency was at the age of 40, you started getting your screening mammograms, and that's just, you have no symptoms. You have nothing going on. You're 40 years old. It's time to get a mammogram. Just like when you turn 50, you got to get a colonoscopy. It's just a way of life. Some people will come in. Well, I feel a mass I'm worried. And this also kind of depends on your age.
Speaker 2:
If you're younger, the chances of you having a mass that's breast cancer is pretty low. You, you may have these little hard nodules called fibroadenomas. They're pretty common in younger people and they grow and shrink in size with your menstrual cycle. And that's something that people usually will point out like, Oh, I noticed this, I know I was on my period last week and now I don't really feel it so much. And so that's, that's pretty common and we can actually do ultrasounds in clinic. I mean, not everyone, but if you're, if the clinic has an ultrasound, we can do an ultrasound because sometimes it's just breast cyst that can feel like a lump and they can hurt. And if it is a cyst, they can drain it in the office and, and hopefully give you some relief. So when you turn 40, get a mammogram, if you feel something that's concerning, you would need to go into your doctor, talk to them about getting an ultrasound or a mammogram.
Speaker 2:
And again, depending on your age, it may dictate what screening that they do. If you have a family history of breast cancer, then that would be something to coordinate with your doctor to get a screening done earlier. They usually recommend doing screening before 40, uh, it may be an MRI and mammogram alternating every six months starting at the age of 25 30. It just kind of depends on when your family member had breast cancer and what genetic mutation it is that you have. So I've had my screening mammogram and I got called back in for more images, do I have cancer? So not necessarily, this is something we actually deal with quite a lot. It really kind of depends on your age and your breast tissue density. It can be really hard to evaluate the breast tissue on a screening mammogram. If you have really dense breast tissue, there's actually, uh, States that have a requirement when they report on your mammogram, that they disclose to you that there are certain regions, depending on the density of your breasts, that they may not be able to see.
Speaker 2:
So they have to give you that information because then if you end up having breast cancer, but you've, you've had a screening mammogram, you know, why wasn't it caught well, and it, it can just really depend on the density of your arrests. So sometimes you'll get a call that you need to come back in and it's for a more formal or what we call a diagnostic mammogram. The difference in that is with a screening mammogram, you kind of just, you go into a facility, they do the mammogram and you go home. And in a couple of days, they either call you with the results or you go into your doctor's office and they give you the results, a diagnostic mammogram, you go into a facility, but the radiologist is, is physically there. And when they do the mammogram, they try and focus on that area that was questionable in your screening mammogram.
Speaker 2:
And so the radiologist can actually look at it in real-time and determine, okay, well, we need a different view here, or we need to zoom in here and take a better look at that so that you don't get called back in for even more. This is, I'm a little bit better idea of, of what they're looking at. And if it, if it is something that looks suspicious for cancer or not, some patients may actually end up needing an ultrasound to go with their mammogram or an MRI. It's all pretty personalized. So it all just depends on what your breast tissue looks like and what, what exactly it is, that's going on, what was seen, or if you're having symptoms and things like that. So it could just be that you have dense breast tissue, and it does not look abnormal when they do the more focused imaging, or could be something that, that is concerning for breast cancer. But being called back does not mean that you have cancer. You could, but they just need to get better pictures. Yeah.
Speaker 1:
Since so, after I got called in my mammogram showed an area concerning for breast cancer and I need a biopsy. Can you explain what that is?
Speaker 2:
Yeah. So when you need a biopsy, it doesn't necessarily mean that it's cancer again. So, so don't panic, but chances are, they saw something that are concerning and suspicious for cancer, and chances are it is, but I need a tissue sample to say for sure what it is. There's different types of breast cancer, there's DCIS, which maybe you've heard of, or there's invasive cancers by doing the biopsy. It gives you a little sample of tissue to be able to determine what type of cancer it is, what hormone receptors it has if it has any. And, and that helps you tailor your treatment, not only for surgery, but if you need chemo or other things, or even additional surgery, when you meet a bias, it can be done a couple of ways, the most common way, or at least the way that I'm used to it being done from when I was in residency is if you have a mask that can be felt if you came in because you had an that you found and you get a mammogram and they, they say, we need to biopsy.
Speaker 2:
If they can see it, then you can get a biopsy done with an ultrasound and you don't have to go through a mammogram again. If you can't see it on an ultrasound, then you got to get a mammogram again. So not, not super fun for everybody when they do it with under a mammogram, it's done by a radiologist typically, and it's called a stereotactic biopsy. So essentially you lay down on this table and you lay face down and there's, there's a little opening in the table. And the breast with the concerning area goes through this little hole in the table and kind of hangs blue so that the arm on this machine can get in the right position and orientation to access the delusion that the arm on the mammogram machine has a needle on it. And once the area is targeted, the needle goes in, they take a sample of the breast tissue that comes out, but there's also a clip that gets placed in the area that they biopsied.
Speaker 2:
So that on later imaging, you can say, okay, well, we already biopsy this area and everything was normal. Or this is where they had a biopsy before we don't see anything different. Or, you know, now there's something there that, that wasn't there before. And we need to re-investigate it. Sometimes you can't do the stereotactic biopsy and that's for reasons, you know, maybe you can't lay flat, maybe it's too uncomfortable, or you can't breathe. There are weight limitations. And depending on your age, I mean, it may just not be something that you're very capable of laying there because it's not, it's not a five-minute procedure. I mean, it's a 20-minute procedure or so. And it depends on where the lesion is. If it's really close to your chest wall, like the muscles underneath your breasts, they don't usually do the stereotactic biopsy. They can still do a biopsy under a mammogram. It's just done a little bit differently. This is all kind of targeted and oriented and one process. Whereas if they have to do it with, without the stereotactic part, it's done a little bit differently. Now there are some stereotactic biopsy machines where you can actually sit up. I don't know how many places have those. Like I don't, I'm not real familiar with how prevalent they are, but they do exist. So that maybe something that they could do.
Speaker 1:
Thank you so much, Dr. Coleman. I know it's a really hard topic to talk about. Cancer is always something that's a pretty scary word. I appreciate you joining us for Talk Tuesdays and telling us what we need to know about breast cancer screening for everyone else. This has been Talk Tuesdays with My Virtual Physician. You can schedule a consultation with one of our doctors by visiting our website: www.myvirtualphysician.com. We look forward to seeing you again, and we hope you have a great week.
Speaker 1 :
Information presented in this podcast is offered for educational purposes, only presenting it is not intended to and does not create a provider-patient relationship between any presenter and anyone else about the medical topics addressed presenters provide general information only not a diagnosis or recommended treatments or any other information specific to any individual listeners are encouraged to see their own healthcare professional about all topics addressed on Talk Tuesdays or for any other medical things.
